| Anaesthesia. 2015 Jan;70 Suppl 1:50-3, e18. |
| The current place of tranexamic acid in the management of bleeding.[Pubmed: 25440395] |
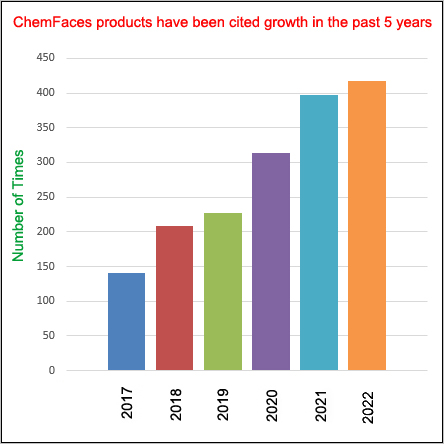
There has been an explosion of interest in the ability of Tranexamic acid to reduce morbidity and mortality in surgical and traumatic bleeding.
METHODS AND RESULTS:
Tranexamic acid has been shown to reduce mortality due to traumatic bleeding by a third, without apparent safety issues. It is now clearly established that intravenous Tranexamic acid reduces blood loss in patients with surgical bleeding and the need for transfusion. It can also be used topically to reduce bleeding. Its use is being explored further in large pragmatic trials in traumatic head injury, postpartum haemorrhage and in upper gastro-intestinal haemorrhage. There are few side effects from the use of Tranexamic acid except when administered in high dose where neurological events have been noted, possibly relating to Tranexamic acid interfering with cerebral GABA and glycine receptors. However, clinical studies suggest that there is no increased efficacy in using a higher dose, and that a dose of 1 g intravenously in an adult patient has maximal efficacy, which is not increased by higher doses.
CONCLUSIONS:
The CRASH-2 trauma trial clearly showed no increase in thrombotic events after its use in trauma, indeed there was a significant reduction in myocardial infarction. However, trials of Tranexamic acid in surgery have failed to adequately study its effects on the risk of postoperative venous and possible reduction in arterial thrombo-embolism, and this needs to be the subject of future research. |
| Arch Orthop Trauma Surg. 2014 Nov;134(11):1609-14. |
| Intravenous use of tranexamic acid reduces postoperative blood loss in total knee arthroplasty.[Pubmed: 25179896] |
Blood transfusion is often required in total knee replacement (TKR); several methods of blood preservation are commonly used but the ideal solution is to reduce the blood loss during and after surgery. Aim of the study was to evaluate the hemostatic efficacy and safety of intravenous use of Tranexamic acid in patients receiving TKR (cemented).
METHODS AND RESULTS:
Forty-five patients after TKR receive treatment with Tranexamic acid (TXA, treatment group), and 45 were managed with fibrin tissue adhesive (control group). Hemoglobin values decrease and transfusions in both groups were recorded. Statistical analysis was performed with Student t test and χ (2) test. A statistical model was elaborated to evaluate together all variables and to underline what data can increase transfusions need.
A significant reduction was detected in hemoglobin values in the first 3 days after surgery in the treatment group. The difference in all cases was significant. When Tranexamic acid was administered, the need for transfusions was lower (difference statistically significant). No major adverse events were recorded in our series. The use of autologous blood preparation before surgery led to a higher transfusion rate.
CONCLUSIONS:
Tranexamic acid reduced blood loss in TKR and significantly reduced the blood transfusion need also when compared to fibrin tissue adhesive. The use of Tranexamic acid is safe and in future may avoid preparation of autologous blood unit before surgery with a decrease of cost and medical figures involved. |
| Br J Anaesth. 2015 Apr;114(4):576-87. |
| Tranexamic acid for the prevention and treatment of postpartum haemorrhage.[Pubmed: 25571934] |
Postpartum haemorrhage (PPH) is a major cause of maternal mortality, accounting for one-quarter of all maternal deaths worldwide. Uterotonics after birth are the only intervention that has been shown to be effective for PPH prevention. Tranexamic acid (TXA), an antifibrinolytic agent, has therefore been investigated as a potentially useful complement to this for both prevention and treatment because its hypothesized mechanism of action in PPH supplements that of uterotonics and because it has been proved to reduce blood loss in elective surgery, bleeding in trauma patients, and menstrual blood loss. This review covers evidence from randomized controlled trials (RCTs) for PPH prevention after caesarean (n=10) and vaginal (n=2) deliveries and for PPH treatment after vaginal delivery (n=1).
CONCLUSIONS:
It discusses its efficacy and side effects overall and in relation to the various doses studied for both indications. TXA appears to be a promising drug for the prevention and treatment of PPH after both vaginal and caesarean delivery. Nevertheless, the current level of evidence supporting its efficacy is insufficient, as are the data about its benefit:harm ratio. Large, adequately powered multicentre RCTs are required before its widespread use for preventing and treating PPH can be recommended. |
| Clin Orthop Relat Res. 2014 May;472(5):1552-7. |
| Topical tranexamic acid reduces blood loss and transfusion rates associated with primary total hip arthroplasty.[Pubmed: 24385043] |
Systemic Tranexamic acid can decrease blood loss and rates of transfusion in patients undergoing total hip arthroplasty (THA). However, the efficacy of topical Tranexamic acid in THA has only recently been characterized in a small number of studies.
The purpose of this study was to compare (1) the greatest hemoglobin decrease after surgery; (2) transfusion rates; and (3) symptomatic thromboembolic events among patients undergoing THA who did and did not receive topical Tranexamic acid.
METHODS AND RESULTS:
We retrospectively compared 135 patients (154 THAs) who received 10 mL 5% Tranexamic acid added in a topical cocktail solution during surgery between January 2009 and July 2011 with 211 patients (234 THAs) who received only the topical cocktail solution (analgesic and antibiotic agent) between January 2005 and December 2008. Contraindications for the use of Tranexamic acid included a documented history of a venous thromboembolic event, an allergy to Tranexamic acid, thrombophilia, or a high risk of venous thromboembolism based on the guidelines of the American Academy of Orthopaedic Surgeons; the 135 patients who received it during that period represented 99.4% of the patients undergoing THA during that time. We compared changes in Hb, transfusion rates, estimated blood loss, surgical results, and complications between the groups. The transfusion threshold was the same, when the Hb values were < 10 g/dL. Patients were screened for thromboembolic disease if symptoms or signs appeared.
Hb decreased less in the Tranexamic acid group (1.87 ± 1.10 g/dL) than in the control group (2.2 ± 1.36 g/dL; p = 0.01) on the first postoperative day. The frequency of transfusion was lower in patients receiving Tranexamic acid (17% as compared with 35% in the control group; p < 0.001). There was only one nonfatal pulmonary embolism in the control group during the study period.
CONCLUSIONS:
Use of topical Tranexamic acid in patients undergoing THA reduces postoperative bleeding and decreases blood transfusion rates. No increase in major complications was identified in patients managed with topical Tranexamic acid. This retrospective study confirms the results of a smaller randomized trial on the same topic by another group. |





 Cell. 2018 Jan 11;172(1-2):249-261.e12. doi: 10.1016/j.cell.2017.12.019.IF=36.216(2019)
Cell. 2018 Jan 11;172(1-2):249-261.e12. doi: 10.1016/j.cell.2017.12.019.IF=36.216(2019) Cell Metab. 2020 Mar 3;31(3):534-548.e5. doi: 10.1016/j.cmet.2020.01.002.IF=22.415(2019)
Cell Metab. 2020 Mar 3;31(3):534-548.e5. doi: 10.1016/j.cmet.2020.01.002.IF=22.415(2019) Mol Cell. 2017 Nov 16;68(4):673-685.e6. doi: 10.1016/j.molcel.2017.10.022.IF=14.548(2019)
Mol Cell. 2017 Nov 16;68(4):673-685.e6. doi: 10.1016/j.molcel.2017.10.022.IF=14.548(2019)

 ACS Nano. 2018 Apr 24;12(4): 3385-3396. doi: 10.1021/acsnano.7b08969.IF=13.903(2019)
ACS Nano. 2018 Apr 24;12(4): 3385-3396. doi: 10.1021/acsnano.7b08969.IF=13.903(2019) Nature Plants. 2016 Dec 22;3: 16206. doi: 10.1038/nplants.2016.205.IF=13.297(2019)
Nature Plants. 2016 Dec 22;3: 16206. doi: 10.1038/nplants.2016.205.IF=13.297(2019) Sci Adv. 2018 Oct 24;4(10): eaat6994. doi: 10.1126/sciadv.aat6994.IF=12.804(2019)
Sci Adv. 2018 Oct 24;4(10): eaat6994. doi: 10.1126/sciadv.aat6994.IF=12.804(2019)